Written by Dr. Dixit Kumar Thakur
| “Delhi’s pollution makes lung infections harder to diagnose than almost anywhere else in India. The chronic airway inflammation from PM2.5 mimics infection symptoms. The weakened lung defences mean infections are more severe. And the city’s unique microbial landscape — TB rates, Aspergillus from dust storms, atypical organisms from urban crowding — means that ‘it’s just a chest infection, take antibiotics’ is the most dangerous thing a Delhi patient can be told. Here’s how I approach it at Pulmovista Clinics.” — Dr. Dixit Kumar Thakur, Senior Pulmonologist, Pulmovista Clinics, Delhi |
I am Dr. Dixit Kumar Thakur, Senior Pulmonologist at Pulmovista Clinics, Delhi. In over 13 years of treating lung infections in this city, I have learned one lesson that I try to share with every patient who sits across from me: in Delhi, lung infections are never straightforward.
Pneumonia, bronchitis, tuberculosis, atypical pneumonia, fungal infection, and pollution-related airway disease can all present with the same basic constellation of symptoms — cough, fever, breathlessness, chest discomfort. But they have completely different causes, completely different treatments, and completely different consequences if mismanaged. The antibiotic that treats bacterial pneumonia does nothing for tuberculosis. The steroid that helps with inflammation can cause catastrophic spread of an undiagnosed fungal infection. Getting the diagnosis right is not a secondary concern — it is the primary clinical task.
This guide walks through how I approach the differential diagnosis of lung infections at Pulmovista Clinics — what distinguishes pneumonia from bronchitis from TB from atypical infections — and what comprehensive lung infection treatment in Delhi looks like when it is done with the precision this city’s respiratory disease environment demands.
1. Why Delhi Makes Lung Infection Diagnosis Uniquely Difficult
Before I explain how I differentiate between infection types, I want to be transparent about something that distinguishes lung infection management in Delhi from anywhere else in India — the factors that make the diagnostic process genuinely harder here:
Factor 1: Pollution Masquerades as Infection
PM2.5 at Delhi’s chronically elevated levels causes airway inflammation, productive cough, breathlessness, and chest discomfort — a clinical picture that is virtually indistinguishable from early bronchitis on history and physical examination alone. Every winter, I see patients at Pulmovista who have been treated with two or three courses of antibiotics for ‘chest infections’ when what they actually had was pollution-driven airway inflammation with no infectious component whatsoever.
The consequences of this misdiagnosis are significant: antibiotic courses that produce no benefit, growing antibiotic resistance from unnecessary prescribing, and — most importantly — failure to address the actual problem, which is the patient’s uncontrolled exposure to PM2.5 and their underlying lung disease that makes them vulnerable to it.
Factor 2: Delhi Has One of the World’s Highest TB Burdens
India carries approximately 27% of the world’s tuberculosis burden. Delhi NCR, with its population density, crowded public transport, migrant worker accommodation, and air quality that impairs lung defences, has TB rates that make it mandatory to consider TB in the differential diagnosis of almost any persistent respiratory presentation. In my clinical practice at Pulmovista, I maintain a very low threshold for TB investigation — because a missed TB diagnosis has consequences that extend far beyond the individual patient.
Factor 3: Aspergillus is Everywhere in Delhi’s Air
Aspergillus mould spores are ubiquitous in Delhi’s environment — present in soil, dust storms, construction debris, and monsoon-humidity indoor environments. For the general population, Aspergillus inhalation is harmless. For patients on corticosteroids, immunosuppressants, or with structural lung disease such as COPD, bronchiectasis, or old TB cavities — Aspergillus can cause invasive pulmonary aspergillosis, a life-threatening infection that is frequently misdiagnosed as bacterial pneumonia and treated with antibiotics that do not touch it.
Factor 4: Antibiotic Resistance Is a Major Clinical Problem
Delhi’s healthcare landscape — a combination of easy over-the-counter antibiotic access, frequent antibiotic prescribing without microbiological guidance, and high patient volume in public health facilities — has created one of the highest rates of antibiotic-resistant organisms in any city in the world. Drug-resistant pneumonia, extended-spectrum beta-lactamase (ESBL)-producing organisms, and multidrug-resistant TB are clinical realities I manage regularly at Pulmovista Clinics. Treating a lung infection empirically — without identifying the organism and its resistance profile — is increasingly inadequate in Delhi’s microbial environment.
| “I tell my patients at Pulmovista that a cough and fever in Delhi requires more thought than a cough and fever in Shimla. Not because Delhi patients are weaker — but because the diagnostic complexity is genuinely higher. The pollution, the TB exposure, the Aspergillus load, the antibiotic resistance — they all change what the ‘chest infection’ in front of me might actually be.” — Dr. Dixit Kumar Thakur, Pulmovista Clinics, Delhi |
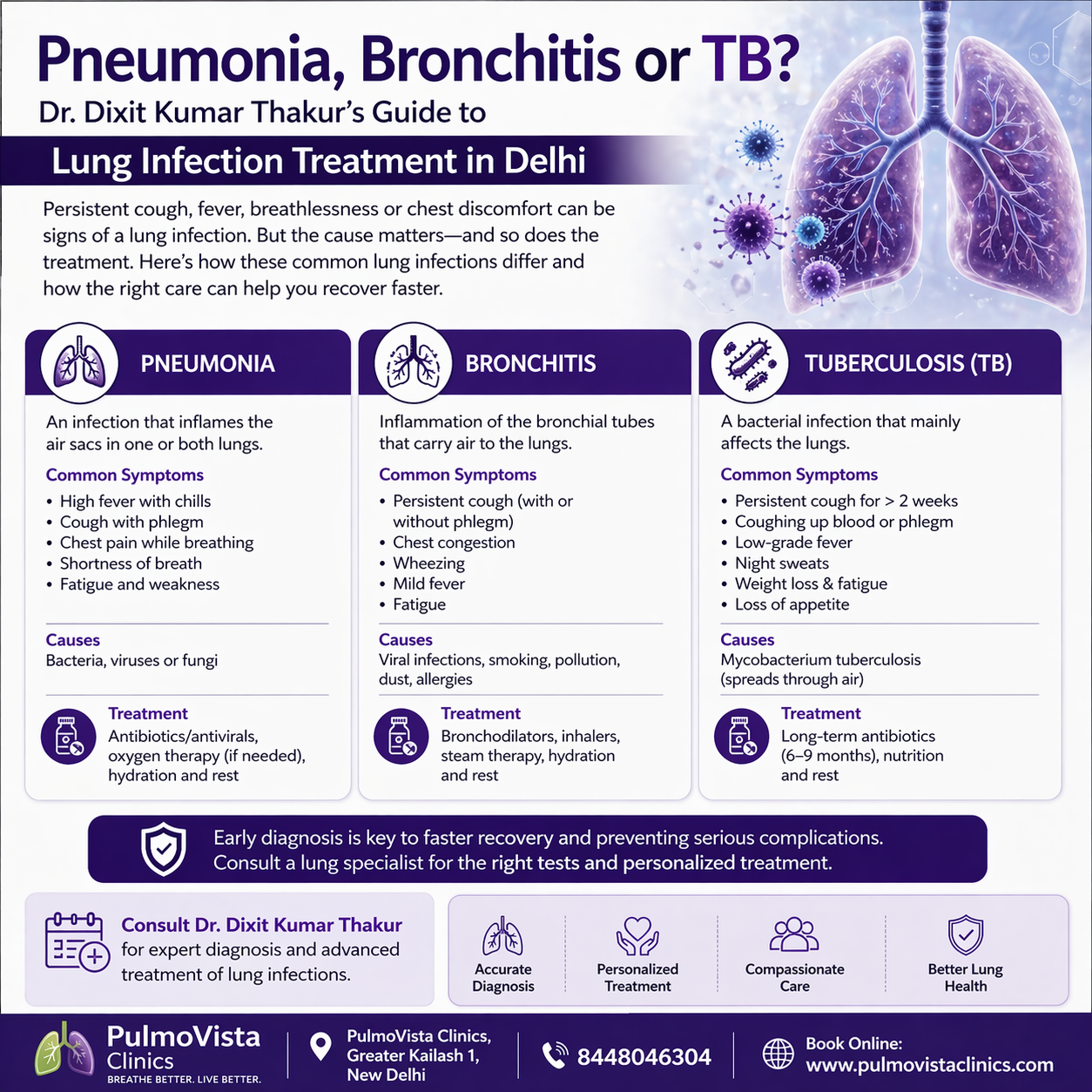
2. The Master Differential: Pneumonia vs. Bronchitis vs. TB vs. Atypical Infection
The central clinical challenge in lung infection treatment in Delhi is differentiating between the major categories of respiratory infection. Here is the master differential diagnosis table I work through at Pulmovista Clinics for every significant respiratory infection presentation:
| Feature | Pneumonia | Acute Bronchitis | Tuberculosis | Atypical / Fungal |
| Onset | Acute (hours–days) | Acute (1–3 days) | Subacute–chronic (weeks–months) | Variable — often subacute |
| Fever | High grade, abrupt | Low grade or absent | Low grade, evening, with night sweats | Variable — may be absent |
| Cough character | Productive, purulent or rusty sputum | Productive, mucoid — clears over 2–3 weeks | Persistent, dry initially then productive; haemoptysis in advanced disease | Dry cough; Aspergillus may cause haemoptysis |
| Breathlessness | Prominent, proportional to affected lung area | Mild — wheeze common | Late feature in primary TB; early in miliary TB | Progressive in invasive aspergillosis |
| Chest X-ray | Lobar or segmental consolidation | Normal or mild hyperinflation | Upper lobe infiltrates, cavitation, hilar lymphadenopathy | Halo sign (aspergillosis); bilateral nodules (fungal); normal (atypical early) |
| Blood tests | High WBC, elevated CRP/ESR, high procalcitonin | Normal or mildly elevated WBC | Elevated ESR/CRP; lymphocytosis; anaemia in chronic disease | Elevated IgE, eosinophilia in ABPA; galactomannan positive in invasive aspergillosis |
| Response to standard antibiotics | Good response in 48–72 hours if correct antibiotic | Antibiotics not indicated — viral aetiology in >90% | No response to standard antibiotics — key diagnostic clue | No response to antibiotics — fungal or atypical |
| Contagion risk | Low (most bacteria not highly contagious) | Low (viral — standard precautions) | HIGH — airborne transmission; contact tracing mandatory | Low (not person-to-person) |
3. Pneumonia in Delhi: How I Diagnose and Treat It at Pulmovista
Community-acquired pneumonia (CAP) is the most common serious lung infection I treat at Pulmovista Clinics. But pneumonia in Delhi is not the textbook presentation from a clean-air city — Delhi’s pollution, antibiotic resistance patterns, and comorbidity burden create a more complex clinical picture that demands a more rigorous approach.
How I Confirm Pneumonia at Pulmovista
• Chest X-ray: The essential first investigation — confirms lobar or segmental consolidation that distinguishes pneumonia from bronchitis, which is a clinical diagnosis based on symptoms with a normal or near-normal chest X-ray.
• Sputum Gram stain and culture: Identifies the causative organism and its antibiotic sensitivity — the cornerstone of targeted therapy. I insist on a sputum culture before prescribing antibiotics for pneumonia at Pulmovista whenever the patient has not already started antibiotics elsewhere.
• Blood cultures: For hospitalised and severe pneumonia — bacteraemia is present in 10–15% of CAP cases and culture-guided therapy significantly improves outcomes.
• Urinary antigen tests: Legionella and Streptococcus pneumoniae urinary antigens provide rapid, non-invasive confirmation of the two most common and most clinically significant CAP pathogens.
• CRP and procalcitonin: Elevated procalcitonin supports bacterial pneumonia over viral or atypical infection — guiding antibiotic decision-making.
• CT chest (selected cases): When the X-ray is non-diagnostic but clinical suspicion is high, when complications are suspected (abscess, effusion), or when the pneumonia fails to resolve as expected.
Pneumonia Severity Assessment: The PSI and CURB-65
One of the most important decisions in pneumonia management is determining whether the patient can be treated safely as an outpatient or requires hospital admission. At Pulmovista Clinics, I use validated severity scoring tools — CURB-65 and the Pneumonia Severity Index (PSI) — to make this decision objectively:
| CURB-65 Score (1 point each) | Management Recommendation |
| C — Confusion (new disorientation) | Score 0–1: Low risk — outpatient treatment appropriate |
| U — Urea >7 mmol/L (or BUN >20mg/dL) | Score 2: Moderate risk — consider short-stay admission or close outpatient follow-up |
| R — Respiratory rate ≥30/min | Score 3–5: High risk — hospital admission required; Score 4–5: consider ICU assessment |
| B — Blood pressure (systolic <90 or diastolic ≤60 mmHg) | At Pulmovista Clinics, scores ≥2 in patients with underlying lung disease prompt hospital referral |
| 65 — Age ≥65 years |
Antibiotic Selection for Pneumonia in Delhi — Why Delhi is Different
Standard CAP antibiotic guidelines are written for populations without Delhi’s resistance profile. At Pulmovista Clinics, my antibiotic prescribing for pneumonia is guided by local resistance data — not just national or international guidelines — because the organisms causing pneumonia in Delhi patients have significantly higher rates of resistance to commonly used antibiotics:
• Streptococcus pneumoniae: Increasing macrolide resistance in Delhi; amoxicillin or amoxicillin-clavulanate remains first-line for outpatient mild-moderate CAP; respiratory fluoroquinolone (levofloxacin, moxifloxacin) for penicillin-allergic patients or macrolide-resistant suspected cases.
• Klebsiella pneumoniae: Classic in Delhi’s diabetic and alcoholic patients — high rates of ESBL production; requires carbapenem or combination therapy in severe cases; sputum culture essential.
• Pseudomonas aeruginosa: In patients with bronchiectasis, COPD, or frequent prior antibiotic courses — requires antipseudomonal coverage (piperacillin-tazobactam, cefepime, or carbapenem); never missed on culture at Pulmovista.
• Atypical organisms (Mycoplasma, Chlamydophila, Legionella): Atypical CAP — particularly in younger, previously healthy patients — requires doxycycline or a respiratory fluoroquinolone. Macrolide resistance in Mycoplasma is emerging in India.
| ⚠ Critical: When Pneumonia Does Not Respond in Delhi If a patient with pneumonia does not show clear clinical improvement within 48–72 hours of appropriate antibiotic therapy, the following must be actively investigated: • Wrong antibiotic — organism resistant to current therapy: sputum culture and sensitivity urgently needed • Wrong diagnosis — could be TB, invasive aspergillosis, or organising pneumonia (COP) rather than bacterial pneumonia • Complication — parapneumonic effusion, empyema, lung abscess — requiring drainage • Impaired host immunity — undiagnosed HIV, haematological malignancy, immunosuppressive medication Non-resolving pneumonia should always prompt a specialist review at Pulmovista Clinics. |
4. Bronchitis in Delhi: The Most Over-Treated Condition I See
Acute bronchitis is the most common respiratory diagnosis in Delhi — and the most over-treated. At Pulmovista Clinics, I estimate that at least 50–60% of the patients I see who have been prescribed antibiotics for ‘chest infection’ actually have acute bronchitis caused by a viral infection — for which antibiotics are completely ineffective and entirely inappropriate.
What Acute Bronchitis Actually Is
Acute bronchitis is inflammation of the bronchial tubes — the large airways — caused in more than 90% of cases by a viral infection: rhinovirus, coronavirus (not SARS-CoV-2 exclusively), influenza, parainfluenza, or RSV. The hallmark is a cough — often productive, often harsh and persistent — that lasts 1–3 weeks, frequently with mild breathlessness and wheeze. The chest X-ray is normal or shows only mild hyperinflation. There is no lobar consolidation.
In Delhi, acute bronchitis is compounded by the chronic low-grade airway inflammation from PM2.5 — meaning that a mild viral bronchitis that would resolve within a week in a clean-air environment can persist for 3–4 weeks in a Delhi resident whose airways are already chronically inflamed. This prolonged course is one of the primary reasons for unnecessary antibiotic prescribing — the patient returns to the physician after 10 days still coughing, and receives a second antibiotic course that does as little as the first.
How I Distinguish Bronchitis from Pneumonia at Pulmovista
• Normal or near-normal chest X-ray: The absence of consolidation is the single most important distinguishing feature. I X-ray every patient with significant respiratory symptoms at Pulmovista — because clinical examination alone cannot reliably exclude pneumonia in Delhi, where comorbidities and pollution dampen the typical clinical signs.
• Normal oxygen saturation: SpO₂ ≥95% at rest — pneumonia typically causes measurable oxygen desaturation; bronchitis generally does not.
• Normal or mildly elevated CRP: Acute bronchitis does not generate the significant systemic inflammatory response that bacterial pneumonia does.
• Symptom timeline: Bronchitis symptoms peak at 3–5 days and gradually improve; pneumonia symptoms typically worsen progressively over the first 48–72 hours without treatment.
Treating Acute Bronchitis — What I Prescribe and Don’t Prescribe
The treatment of viral acute bronchitis does not include antibiotics. At Pulmovista Clinics, my management of acute bronchitis involves:
• Short-acting bronchodilator (Salbutamol): For wheeze and breathlessness — provides symptomatic relief while the viral infection resolves.
• Ipratropium bromide: Can reduce cough severity in acute bronchitis — evidence-supported.
• Mucolytic agents: N-acetylcysteine or carbocisteine — reduce mucus viscosity and ease expectoration.
• Adequate hydration: Maintaining fluid intake reduces mucus viscosity and supports mucociliary clearance.
• Honey and warm fluids: Evidence-supported soothing of airway irritation — particularly useful for night cough.
• Delayed antibiotic prescription: For patients who are very anxious about not receiving antibiotics, I sometimes provide a delayed prescription — to be filled only if there is no improvement after 5–7 days. Studies show this reduces actual antibiotic use by 70% without compromising outcomes.
5. Tuberculosis in Delhi: The Diagnosis That Cannot Be Missed
In over 13 years of pulmonology practice in Delhi, tuberculosis remains the diagnosis I am most vigilant about — because the consequences of a missed TB diagnosis extend far beyond the individual patient. A patient with undiagnosed pulmonary TB walking through Delhi’s crowded metro, buses, and markets can infect dozens of contacts. And drug-resistant TB — which is increasing in Delhi — becomes progressively harder and more expensive to treat with every missed diagnostic opportunity.
Who I Consider for TB Investigation at Pulmovista
At Pulmovista Clinics, I maintain a very low threshold for TB investigation. Any patient with the following should be investigated for TB — regardless of how their presentation is initially labelled:
| 📋 Pulmovista Clinics TB Investigation Threshold — Any of the Following Warrants Testing 📋 Cough lasting more than 2–3 weeks — particularly if productive 📋 Unexplained weight loss of 5% or more over 2–3 months 📋 Low-grade fever — particularly evening fever with night sweats 📋 Haemoptysis (coughing up blood) — even a single episode 📋 Fatigue and loss of appetite without another explanation 📋 Chest X-ray showing upper lobe infiltrates, cavitation, or hilar lymphadenopathy 📋 Pneumonia that has not responded to 2 or more appropriate antibiotic courses 📋 Known TB contact in household, workplace, or social setting 📋 Immunocompromised patient — HIV, on corticosteroids, on TNF inhibitors, post-transplant 📋 Recent migration from high-TB burden areas; healthcare worker with occupational exposure |
How I Investigate for TB at Pulmovista
• Sputum AFB smear and culture (3 samples on 3 consecutive days): The first-line microbiological test — sputum stained for acid-fast bacilli. Culture takes 2–6 weeks but provides drug sensitivity information essential for treatment planning.
• CBNAAT / GeneXpert MTB/RIF: Rapid molecular test detectable within 2 hours — identifies Mycobacterium tuberculosis and rifampicin resistance simultaneously. This is the test I order first at Pulmovista when TB is clinically suspected, because speed of diagnosis matters enormously for infection control.
• Chest X-ray and HRCT: Chest X-ray identifies classic upper lobe infiltrates, cavitation, and miliary pattern. HRCT provides more detail — particularly useful for smear-negative TB and for assessing the extent of disease.
• Mantoux test (TST) and IGRA (QuantiFERON): Immunological tests for TB infection — positive results indicate TB infection but do not distinguish active from latent TB. Most useful in contact investigation and in immunocompromised patients where sputum testing may be negative.
• Bronchoscopy with BAL: For smear-negative patients unable to produce sputum — bronchoalveolar lavage for AFB smear, culture, and GeneXpert.
• Drug sensitivity testing (DST): All TB isolates at Pulmovista are tested for first-line (isoniazid, rifampicin, pyrazinamide, ethambutol) and second-line drug resistance — given Delhi’s high MDR-TB prevalence.
TB Treatment at Pulmovista Clinics
TB treatment in India follows RNTCP/NTEP (National TB Elimination Programme) protocols. At Pulmovista Clinics, I manage TB treatment with the following principles:
• Drug-sensitive TB: 6-month standard regimen — 2 months of HRZE (isoniazid, rifampicin, pyrazinamide, ethambutol) followed by 4 months of HR (isoniazid, rifampicin). Nikshay registration mandatory for all TB patients in India.
• Drug-resistant TB: MDR-TB (resistant to rifampicin and isoniazid) requires specialist management with second-line drugs. I refer all confirmed MDR-TB patients to a designated MDR-TB treatment centre with my detailed clinical notes — ensuring continuity of care.
• Treatment adherence: The biggest challenge in TB treatment is completing the full 6-month course. At Pulmovista Clinics, I monitor adherence at every visit, educate patients about the consequences of incomplete treatment (drug resistance development), and link patients with adherence support resources.
• Post-TB lung disease: Many patients at Pulmovista present with residual lung damage from previous TB — bronchiectasis, pleural thickening, lung fibrosis. I assess and manage these sequelae with spirometry, HRCT, and — where significant functional impairment is present — pulmonary rehabilitation.
6. Atypical Pneumonia and Fungal Infections: The Diagnoses Delhi Keeps Missing
Atypical Pneumonia — Walking Pneumonia in Delhi
Atypical pneumonia — caused by Mycoplasma pneumoniae, Chlamydophila pneumoniae, and Legionella pneumophila — presents very differently from typical bacterial pneumonia. It is sometimes called ‘walking pneumonia’ because patients are often ambulatory and relatively well-appearing despite significant pulmonary infiltrates on chest X-ray. The classic presentation:
• Gradual onset over 1–2 weeks rather than the abrupt onset of typical bacterial pneumonia
• Dry, persistent, non-productive cough in contrast to the purulent sputum of pneumococcal pneumonia
• Patchy bilateral infiltrates on chest X-ray — often more extensive than the clinical picture would suggest
• Poor response to beta-lactam antibiotics — Mycoplasma and Chlamydophila lack cell walls and are intrinsically resistant to penicillins and cephalosporins
• Extrapulmonary features in Mycoplasma — rash, haemolytic anaemia, neurological symptoms
Atypical pneumonia requires doxycycline or a respiratory fluoroquinolone — not the amoxicillin or co-amoxiclav typically prescribed for CAP. This is one of the most common prescribing errors I correct at Pulmovista.
Legionella Pneumonia — The Air Conditioning Risk in Delhi’s Commercial Buildings
Legionella pneumophila causes a severe atypical pneumonia transmitted through contaminated water aerosols — most commonly from cooling towers, air conditioning systems, and hot water systems in hotels, hospitals, and large commercial buildings. South Delhi’s large hotel and commercial sector, combined with aging air conditioning infrastructure, creates genuine Legionella exposure risk.
Legionella pneumonia is clinically severe — high fever, confusion, abdominal symptoms, markedly elevated CRP and hyponatraemia. The urinary Legionella antigen test (available at Pulmovista Clinics) provides rapid diagnosis. Treatment is a fluoroquinolone or azithromycin — beta-lactams are ineffective.
Aspergillus Infections in Delhi — A Spectrum of Disease
Aspergillus species cause a spectrum of pulmonary disease depending on the patient’s immune status and underlying lung condition. At Pulmovista Clinics, I identify and manage all three major Aspergillus clinical syndromes:
| Aspergillus Syndrome | Who Gets It | How I Diagnose and Treat at Pulmovista |
| ABPA (Allergic Bronchopulmonary Aspergillosis) | Asthma or CF patients with Aspergillus sensitisation | Total IgE >1000 IU/mL; Aspergillus-specific IgE; precipitins; HRCT shows central bronchiectasis and mucus plugging. Treatment: oral prednisolone + itraconazole; Omalizumab for refractory cases. |
| Aspergilloma (Fungal Ball) | Old TB cavities, healed lung abscesses — structural lung disease | HRCT shows fungal ball within a pre-existing cavity — the ‘air crescent sign.’ May cause haemoptysis. Treatment: monitoring for stable disease; antifungal or surgical referral for haemoptysis. |
| Invasive Pulmonary Aspergillosis (IPA) | Immunocompromised patients — neutropenia, steroids, post-transplant, haematological malignancy | HRCT halo sign (ground-glass opacity surrounding nodule). Serum galactomannan. BAL culture. Treatment: urgent voriconazole or isavuconazole — a medical emergency requiring immediate specialist management. |
7. My Diagnostic Framework at Pulmovista: How I Approach Every Lung Infection in Delhi
After 13 years of lung infection treatment in Delhi, I have developed a systematic diagnostic framework that I apply to every significant respiratory infection presentation at Pulmovista Clinics. This framework is designed specifically for Delhi’s complex microbial and pollution environment — not for a clean-air clinical setting.
1. History first — always: Duration of symptoms, character of cough, sputum colour and quantity, fever pattern (abrupt high-grade vs. low-grade evening), night sweats, weight loss, haemoptysis, recent travel, TB contacts, immunosuppressive medications, occupation, and — critically — previous antibiotic courses and their response.
2. X-ray before antibiotics — whenever possible: I do not prescribe antibiotics for a ‘chest infection’ without a chest X-ray at Pulmovista. The X-ray separates pneumonia from bronchitis, identifies TB-suspicious patterns, reveals complications, and provides an objective baseline for monitoring response.
3. Sputum culture — not optional for significant infections: Empirical antibiotic therapy is a starting point, not a substitute for microbiological diagnosis. At Pulmovista, I insist on a sputum Gram stain, culture, and AFB smear in every patient with significant or persistent respiratory infection — before antibiotics if possible, immediately after if the clinical urgency does not allow delay.
4. TB in the differential — always: I consciously place TB on the differential diagnosis for every respiratory presentation lasting more than 2 weeks in Delhi. The stigma and delays associated with TB diagnosis in India mean that many patients have already seen 2–3 clinicians before reaching Pulmovista — and TB was not considered because no one thought to ask the right questions.
5. Consider the immunological context: Is this patient immunocompromised? On corticosteroids? HIV positive? Diabetic with poor glycaemic control? Immunocompromise completely changes the diagnostic differential — Aspergillus, Pneumocystis, atypical mycobacteria, and viral pneumonias all become possibilities that are uncommon in immunocompetent patients.
6. Non-response protocol: If a patient does not improve within 48–72 hours on appropriate antibiotic therapy, I follow a structured non-response protocol — repeat imaging, culture review, consideration of TB or fungal investigation, and specialist respiratory review. I never simply change to a different antibiotic without understanding why the first one failed.
7. Pollution as a confounding factor: I always ask: is this a true infection or pollution-driven airway disease mimicking infection? Spirometry, CRP, and the clinical response to bronchodilators versus antibiotics help distinguish the two — and prevent the cycle of unnecessary antibiotic prescribing that I see in so many of my referred patients.
8. Why Delhi Patients Trust Pulmovista Clinics for Lung Infection Treatment in Delhi
When Delhi patients or their families search for expert lung infection treatment in Delhi — after being told their pneumonia has not resolved, or after a third antibiotic course with no improvement, or after a TB diagnosis that was delayed for months — Pulmovista Clinics is the destination they find. Here is what makes the difference:
1. Microbiological precision: At Pulmovista, antibiotic prescriptions are guided by sputum culture and sensitivity results — not by protocol alone. In Delhi’s antibiotic-resistance landscape, this precision is clinically critical and often the difference between treatment success and failure.
2. Active TB vigilance: TB is on my differential diagnosis for every persistent respiratory presentation at Pulmovista. I have identified TB in patients who had been treated for ‘pneumonia’ or ‘bronchitis’ for months — because I ask the right questions and order the right tests rather than assuming a bacterial aetiology.
3. Fungal infection expertise: ABPA, aspergilloma, and invasive aspergillosis are conditions I diagnose and manage regularly at Pulmovista Clinics — because Delhi’s Aspergillus exposure and the prevalence of predisposing conditions (asthma, old TB cavities, structural lung disease) make these diagnoses genuinely common.
4. Full diagnostic infrastructure: HRCT chest, bronchoscopy, BAL for microbiological sampling, GeneXpert for rapid TB diagnosis, Legionella and pneumococcal urinary antigens, complete blood panel including procalcitonin and galactomannan — all accessible through Pulmovista Clinics.
5. Non-resolving pneumonia assessment: For patients referred with pneumonia that has not cleared despite treatment — a structured, systematic investigation to identify the true diagnosis: organising pneumonia, bronchial obstruction, ABPA, TB, or resistant organism infection.
6. Post-infection lung damage management: Following severe pneumonia, TB, or COVID-19, many patients develop residual lung damage — bronchiectasis, fibrosis, reduced exercise capacity. At Pulmovista Clinics, I assess and manage post-infection lung sequelae with spirometry, HRCT, and — where functional impairment is significant — pulmonary rehabilitation.
Conclusion: In Delhi, Precision Matters More Than Speed
Delhi’s lung infection landscape is unlike any other city in India. Pollution that mimics infection. TB that hides behind repeated antibiotic courses. Aspergillus from the air itself. Antibiotic-resistant organisms from decades of over-prescribing. The correct response to this complexity is not faster antibiotic prescribing — it is more precise diagnosis.
At Pulmovista Clinics, Dr. Dixit Kumar Thakur brings 13 years of Delhi-specific respiratory expertise, a full diagnostic infrastructure, and a systematic clinical framework to every lung infection presentation. Not every cough needs an antibiotic. Not every ‘chest infection’ is bacterial. And no pneumonia that fails to respond to treatment should be treated with a second antibiotic before the first diagnosis has been rigorously questioned.
If you have a lung infection that is not resolving, a cough that has been present for weeks, or a TB question that no one has yet answered — book your consultation at Pulmovista Clinics today.
FAQs-Lung Infections and Diagnosis in Delhi
- How do I know if I have pneumonia or just bronchitis?The most reliable way is a chest X-ray — pneumonia shows consolidation (a dense shadow in the lung parenchyma) while bronchitis typically shows a normal or near-normal X-ray. Clinically, pneumonia tends to cause higher fever, more significant breathlessness, and oxygen desaturation — but these features overlap. At Pulmovista Clinics, I X-ray every patient with significant respiratory symptoms before prescribing antibiotics, because clinical examination alone cannot reliably make this distinction in Delhi, where pollution and underlying lung disease complicate the picture.
- I have been coughing for 4 weeks. Should I be tested for TB?Yes. Any cough lasting more than 3 weeks in Delhi should be investigated for TB — and at Pulmovista Clinics, I consider TB investigation for any cough beyond 2 weeks in a patient with other risk factors (weight loss, night sweats, TB contact, immunocompromise). The test is simple — a sputum sample for GeneXpert MTB/RIF provides a result within hours. A chest X-ray is also essential. Please do not wait for a haemoptysis or weight loss to seek TB investigation — early diagnosis produces far better outcomes and prevents transmission.
- My doctor gave me antibiotics for a chest infection but I am no better after 5 days. What should I do?Seek a specialist review at Pulmovista Clinics immediately. Non-response to antibiotics at 48–72 hours is a clinical warning sign — it may indicate the wrong antibiotic for the organism, a resistant organism, the wrong diagnosis (TB, ABPA, viral infection, organising pneumonia), or a complication (lung abscess, empyema). Simply switching to a different antibiotic without investigation is not appropriate. At Pulmovista, non-response triggers a systematic review: repeat imaging, sputum culture, TB investigation, and clinical reassessment.
- Can Delhi's pollution cause symptoms that look like a lung infection?Absolutely — and this is one of the most important diagnostic distinctions I make at Pulmovista Clinics every week. Chronic PM2.5 exposure causes airway inflammation that produces cough, breathlessness, and sputum production that is clinically indistinguishable from early bronchitis or mild pneumonia on history alone. This is why Delhi patients are among the most antibiotic-over-treated in the world — pollution symptoms are routinely diagnosed as chest infections and treated with antibiotics that provide no benefit. A chest X-ray, CRP, and the clinical response to bronchodilators versus antibiotics help me distinguish true infection from pollution-driven airway inflammation at Pulmovista.
- How do I book a lung infection assessment at Pulmovista Clinics?You can book a consultation with Dr. Dixit Kumar Thakur at Pulmovista Clinics by visiting www.pulmovista.com or calling the clinic directly. Both in-person and teleconsultation appointments are available. When booking, please mention the duration of your symptoms and any previous investigations or antibiotic courses — this helps me arrange the appropriate tests (chest X-ray, sputum culture, GeneXpert) before or at your appointment. For patients with non-resolving pneumonia or suspected TB, please request an urgent appointment.