Written by Dr. Dixit Kumar Thakur
| “Use this 5-question checklist before your next consultation at Pulmovista Clinics — because the answer to every question tells me something about whether your asthma medications are actually working. Most patients arrive at my clinic believing their medications are fine. The checklist tells a different story.” — Dr. Dixit Kumar Thakur, Senior Pulmonologist, Pulmovista Clinics, Delhi |
I am Dr. Dixit Kumar Thakur, Senior Pulmonologist at Pulmovista Clinics, Delhi. Every week, patients sit across from me having taken the same asthma medications for years — sometimes the same blue rescue inhaler since childhood — without ever being asked a single question about whether those medications are actually doing what they are supposed to do.
This is the central problem with asthma management in India today: medications are prescribed, but control is never objectively assessed. The inhaler is handed over, the patient leaves, and the assumption is made that if they have not been admitted to hospital, the treatment is ‘working.’ This assumption is wrong — and it is costing patients their quality of life, their lung health, and in some cases, their lives.
The five questions in this guide are the ones I ask every asthma patient at their first appointment at Pulmovista Clinics. They are drawn directly from the GINA 2026 (Global Initiative for Asthma) assessment framework — the international gold standard for evaluating asthma control. They are simple, honest, and take less than two minutes to answer. And they will tell you — and me — whether your current asthma medications in Delhi are working the way they should.
Work through each question honestly. Then read what your answers mean. And if the checklist reveals what I suspect it will for many of you — book a consultation at Pulmovista Clinics. Because the asthma medications available in 2026, used correctly and prescribed by a specialist who understands your specific disease, are capable of giving you a level of control you may have stopped believing is possible.
Before the Questions: Why Asthma Medication Assessment Matters So Much in Delhi
Before I walk you through the five questions, I want to establish something that fundamentally shapes how I approach asthma medications in Delhi — something that distinguishes managing asthma in this city from managing it anywhere else in India.
Delhi’s air quality is not a background variable in asthma management. It is an active, chronic, year-round clinical factor that changes the biology of asthma and the performance of asthma medications in ways that most patients — and many general physicians — do not fully appreciate:
• PM2.5 causes partial steroid resistance: Chronic exposure to fine particulate matter drives neutrophilic airway inflammation that responds poorly to inhaled corticosteroids (ICS) — the cornerstone of standard asthma controller therapy. Asthma medications that work well in clean-air environments may provide significantly less control in Delhi.
• SABA overuse is dangerously common: The most widely prescribed asthma medication in Delhi remains Salbutamol (blue rescue inhaler) — used alone, without any anti-inflammatory controller. GINA 2026 explicitly states that SABA-only therapy is no longer recommended at any severity level. Yet the majority of Delhi asthma patients are on it.
• Allergen burden amplifies medication failure: Delhi’s year-round high dust mite, Prosopis pollen, Aspergillus mould, and cockroach allergen burden creates a chronic allergic trigger load that overwhelms standard ICS therapy in sensitised patients — making them appear ‘medication-resistant’ when in fact they need targeted allergen management and potentially biologic therapy.
• Seasonal peaks expose hidden inadequacy: Many patients believe their asthma medications are working because they feel ‘fine’ in summer. Then October arrives — stubble burning, inversions, Diwali — and they end up in the emergency department. The medications were not working. The season was just forgiving.
| “Asthma medications in Delhi must be evaluated against Delhi’s air — not against clean-air clinical trial conditions. A medication regimen that would control asthma in Shimla may be completely inadequate for the same patient in South Delhi during November. This is one of the most important things I discuss at Pulmovista Clinics with every asthma patient.” — Dr. Dixit Kumar Thakur, Pulmovista Clinics, Delhi |
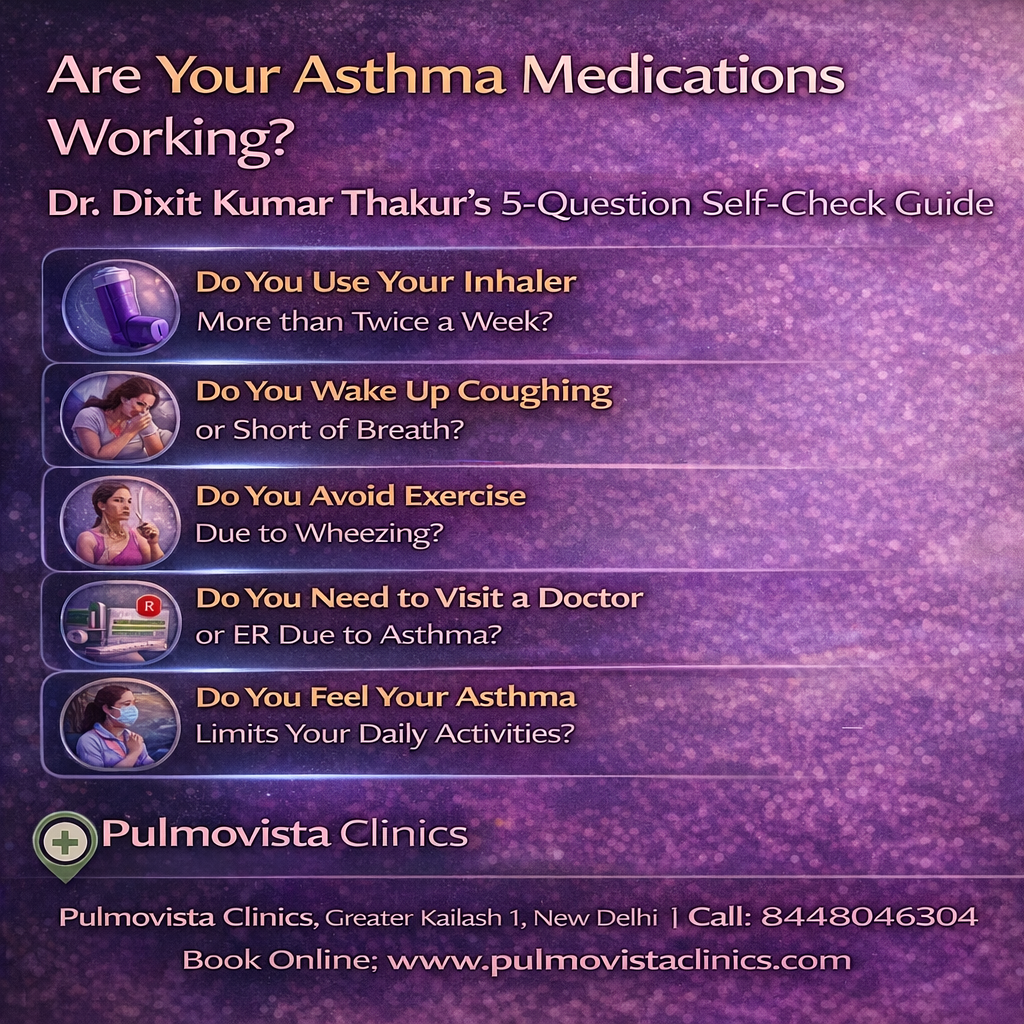
The 5-Question Self-Check: Use This Before Your Next Pulmovista Consultation
| 📋 How to Use This Checklist Answer each question honestly based on the past 4 weeks. For each question, the YES answer reflects adequate asthma control for that parameter. The NO answer reflects a specific control failure that needs to be addressed. At the end, count your NO answers. Each NO is a signal — not a label. Share your answers with Dr. Dixit Kumar Thakur at your next Pulmovista Clinics appointment. This checklist is based on the GINA 2026 Asthma Control Assessment Tool — the international gold standard for evaluating whether asthma medications are working. |
| QUESTION 1: In the past 4 weeks, have you had daytime asthma symptoms on FEWER than 2 days per week? ☐ YES: Daytime symptoms on 2 or fewer days per week — this specific parameter is controlled. ☐ NO: Daytime symptoms on more than 2 days per week — your asthma medications are not adequately controlling daytime inflammation. Dr. Thakur’s Verdict: Daytime symptoms more than twice a week is the GINA 2026 definition of uncontrolled asthma for this parameter. It means your controller medications — whatever they are — are not suppressing airway inflammation adequately. The most common reasons I find at Pulmovista: SABA-only therapy with no controller; ICS prescribed but taken irregularly; incorrect inhaler technique meaning medication never reaches the lungs; or asthma severity that has outgrown the current treatment step. |
Why Daytime Symptom Frequency Matters: The Clinical Explanation
Every day you have asthma symptoms, your airways are inflamed. Every symptom episode — every wheeze, every chest tightness, every unexplained cough — is airway inflammation expressing itself clinically. The goal of asthma controller medications is not to provide relief when symptoms occur. It is to suppress the underlying inflammation so thoroughly that symptoms do not occur in the first place.
If you are symptomatic on more than 2 days per week despite being on asthma medication, one of the following is true: you are not on a controller medication at all (SABA-only therapy); you are on a controller medication but using it incorrectly or irregularly; your controller medication dose is too low for your level of inflammation; or your asthma phenotype requires a different class of medication altogether — which only a specialist assessment with FeNO testing and allergy evaluation can determine.
| QUESTION 2: In the past 4 weeks, have you used your rescue inhaler (Salbutamol/blue inhaler) on FEWER than 2 days per week? ☐ YES: Rescue inhaler used on 2 or fewer days per week — rescue medication use is within the controlled range. ☐ NO: Rescue inhaler used on more than 2 days per week — this is one of the clearest signals that asthma medications are failing. Dr. Thakur’s Verdict: Rescue inhaler use more than twice per week is the single most important and most widely ignored warning sign in asthma management. At Pulmovista Clinics, when I ask patients how often they use their blue inhaler, the most common answer is ‘every day’ — often multiple times. And they have been doing this for years, believing it is normal. It is not normal. It is a sign of uncontrolled asthma requiring immediate medication review. GINA 2026 states unequivocally: frequent SABA use is a marker of poor control and a risk factor for life-threatening asthma attacks. |
The Rescue Inhaler Trap: What I See Every Week at Pulmovista
The rescue inhaler trap is one of the most common and most dangerous patterns I encounter in asthma management across Delhi. It works like this: a patient is given a Salbutamol inhaler at their first asthma diagnosis. It works immediately — bronchospasm relieved, breathlessness gone. So they use it every time they have symptoms. And it works every time. So they conclude their asthma is under control.
It is not. Salbutamol relaxes the smooth muscle around the airways, providing temporary bronchodilation. But it has zero anti-inflammatory effect. Every time the Salbutamol wears off, the underlying airway inflammation reasserts itself — causing the next episode of symptoms. The patient takes another puff. Temporary relief. Inflammation continues. Airway remodelling progresses. Years pass. The patient uses their blue inhaler multiple times every day and considers this normal management.
It is not management. It is symptom suppression without disease control — and over time, it allows airway remodelling that makes the asthma progressively harder to treat. The asthma medications needed in this situation are not more Salbutamol. They are controller medications that address the inflammation — specifically, SMART therapy (ICS-formoterol) as recommended by GINA 2026.
| QUESTION 3: In the past 4 weeks, have you been free from nighttime waking or early-morning symptoms caused by asthma? ☐ YES: No nighttime waking or early-morning symptoms — nocturnal asthma control is adequate. ☐ NO: Waking at night or experiencing symptoms in the early morning due to asthma — a critical signal of inadequate overnight inflammation control. Dr. Thakur’s Verdict: Nocturnal symptoms are one of the most important asthma control indicators — and one of the most frequently normalised by patients who have lived with them for years. At Pulmovista Clinics, I regularly see patients who describe waking at 2am with cough or wheeze as ‘just something that happens’ — not recognising it as a sign that their asthma medications are failing overnight. Nocturnal symptoms indicate that the anti-inflammatory effect of their controller medication has worn off by the early hours — or was never adequate to begin with. In Delhi, where PM2.5 exposure continues even indoors through the night in homes without HEPA purifiers, nocturnal inflammation burden is particularly high. |
Why Asthma Is Worst at Night: The Biology
Nocturnal asthma is not random. It follows a predictable circadian pattern driven by several well-understood biological mechanisms:
• Cortisol nadir: Natural cortisol levels fall to their lowest point between 2am and 4am — reducing the endogenous anti-inflammatory signal that partially suppresses airway inflammation during the day. This cortisol trough is why most nocturnal asthma attacks occur in the small hours.
• Airway cooling: Lying horizontal reduces the effect of gravity on the chest wall and slightly increases airway resistance. Combined with cooler nocturnal temperatures in Delhi (particularly in winter), this promotes airway narrowing.
• Allergen exposure: Bedroom allergen loads — house dust mite in mattresses and pillows, mould if humidity is not controlled — are particularly high. Prolonged 7–8 hour nocturnal exposure to these allergens without the activity-related airway protection of daytime movement amplifies nocturnal inflammation.
• Gastro-oesophageal reflux: GERD is most active in the supine position — nocturnal acid reflux into the oesophagus triggers bronchoconstriction through vagal reflex pathways, causing nocturnal symptoms that are incorrectly attributed to asthma alone rather than to the GERD-asthma interaction.
| QUESTION 4: In the past 4 weeks, have your asthma symptoms caused NO limitation to your daily activities, exercise, work, or social life? ☐ YES: No activity limitation due to asthma — this control parameter is met. ☐ NO: Any limitation to daily activities, exercise, work, or social life due to asthma — your medications are not achieving full asthma control. Dr. Thakur’s Verdict: Activity limitation is the control parameter that patients most commonly accept and adapt to without recognising it as a medication failure. I see it constantly at Pulmovista Clinics: the patient who stopped swimming because ‘my asthma doesn’t like it.’ The professional who works from home on high-pollution days because going to the office triggers symptoms. The parent who sends a friend to pick up children from school on dusty days. The retired person who has quietly stopped visiting the market, attending functions, or taking morning walks. These are not lifestyle choices. They are signs that asthma medications are failing. Fully controlled asthma should allow essentially normal daily activities — with appropriate environmental precautions on extreme pollution days. |
Activity Limitation and Asthma: What ‘Accepted Normal’ Actually Signals
The most insidious form of asthma undertreatment is the kind that is invisible — where patients have quietly shrunk their lives around their asthma without recognising the shrinkage as abnormal. Over months and years, the distance walked gets shorter. The social events attended get fewer. The stairs taken get avoided. The exercise abandoned.
This gradual life-contraction is one of the most powerful arguments for objective asthma assessment. If I only ask ‘how are your symptoms?’ patients often say ‘not bad’ — because they have adjusted their life so that they rarely encounter the activities that would provoke symptoms. It is only when I ask the activity limitation question specifically — ‘have you stopped doing anything because of your asthma?’ — that the full picture emerges.
At Pulmovista Clinics, restoring activity capacity is one of the primary treatment goals I set for every patient. Not just suppressing symptoms — but enabling the life that was shrinking. When the right asthma medications are combined with SMART therapy, allergen management, and where necessary biologic therapy, the restoration of activity capacity is one of the most gratifying clinical outcomes I witness.
| QUESTION 5: In the past 4 weeks, have you had NO severe asthma attacks (exacerbations) requiring oral steroids, emergency care, or hospitalisation? ☐ YES: No severe exacerbations in the past 4 weeks — exacerbation control is met for this period. ☐ NO: One or more severe asthma exacerbations in the past 4 weeks requiring oral steroids, emergency care, or hospitalisation — this is the most critical signal of medication failure. Dr. Thakur’s Verdict: A severe asthma exacerbation is not ‘bad luck.’ It is a definitive signal that current asthma medications are insufficient to protect the patient from acute disease escalation. At Pulmovista Clinics, every patient who presents following a severe exacerbation undergoes a formal medication review and step-up assessment — because GINA 2026 is clear: one severe exacerbation in a year is grounds for stepping up therapy; two or more is grounds for biologic therapy assessment. Severe exacerbations are also cumulative events — each one causes airway remodelling that makes future exacerbations more likely and harder to treat. The only acceptable response to a severe exacerbation is a specialist review and medication upgrade. |
Why Exacerbations Are Never ‘Just One Bad Episode’
One of the most important reframes I offer patients at Pulmovista Clinics is this: a severe asthma exacerbation is not an isolated event. It is a marker of ongoing medication inadequacy — and it leaves a scar. Each severe exacerbation causes a measurable, lasting reduction in FEV₁. Patients who have repeated exacerbations have faster lung function decline than patients whose asthma is controlled. The airways are structurally remodelled by each severe inflammatory episode — thickening of the bronchial wall, increased smooth muscle mass, mucus gland hypertrophy — changes that progressively reduce responsiveness to treatment.
This is why the GINA 2026 framework does not treat exacerbations as unfortunate background noise. They are clinical events requiring a formal response — a step-up in asthma medications, a specialist review, and in patients with two or more per year, a structured assessment for biologic therapy at a centre equipped to provide it, such as Pulmovista Clinics.
Interpreting Your Score: What Your Answers Tell Dr. Dixit Kumar Thakur
| NO Answers | Asthma Control Level | What This Means & What to Do |
| 0 NO answers (all 5 YES) | WELL CONTROLLED | Your asthma medications appear to be working adequately for the past 4 weeks. Annual review at Pulmovista Clinics is still recommended — sustained control warrants a step-down assessment to the minimum effective medication dose. |
| 1–2 NO answers | PARTLY CONTROLLED | Your asthma medications are providing partial but incomplete control. A medication review and possible step-up is indicated. Book a consultation at Pulmovista Clinics — the specific questions you answered NO to direct my assessment toward the most likely inadequacy. |
| 3–5 NO answers | UNCONTROLLED | Your asthma medications are clearly not working adequately. This is not bad luck and it is not the best you can expect. Uncontrolled asthma in 2026 is a treatable condition. Book an urgent consultation at Pulmovista Clinics — complete spirometry, FeNO testing, allergy evaluation, and SMART therapy assessment are the immediate priorities. |
| Any answer includes a recent severe exacerbation | HIGH RISK — URGENT REVIEW | Regardless of your other answers, a recent severe exacerbation requiring oral steroids, emergency care, or hospitalisation requires immediate specialist review. Do not wait for your next scheduled appointment. Contact Pulmovista Clinics for an urgent consultation. |
What ‘Working’ Asthma Medications Actually Look Like: The GINA 2026 Standard
Many patients have never been told what well-controlled asthma is supposed to feel like. They have accepted a level of daily symptoms, rescue inhaler use, and activity limitation that feels normal — because it has been their normal for years. Here is the GINA 2026 definition of well-controlled asthma that I use as the target for every patient at Pulmovista Clinics:
| ✅ Well-Controlled Asthma — The Target Dr. Dixit Kumar Thakur Sets for Every Pulmovista Patient ✅ Daytime symptoms on 2 or fewer days per week ✅ No nighttime waking or early-morning symptoms due to asthma ✅ Rescue inhaler use on 2 or fewer days per week ✅ No limitation to daily activities, exercise, work, or social life ✅ Normal or near-normal lung function (FEV₁ ≥80% predicted) ✅ FeNO within target range for current ICS dose — confirmed by objective measurement at Pulmovista ✅ No severe exacerbations in the past 12 months ✅ Minimal side effects from asthma medications This level of control is achievable for the vast majority of asthma patients — with the right medications, correctly prescribed and correctly used. |
Asthma Medications in Delhi in 2026: What the Options Are
If this checklist has revealed that your current asthma medications in Delhi are not working as well as they should, the next question is: what should they be changed to? Here is my complete overview of the asthma medication options available in 2026, and when each one is appropriate — explained in plain language:
Step 1: As-Needed Low-Dose ICS-Formoterol (New GINA 2026 First Line)
The most important change in GINA 2026 — one that most Delhi patients and many GPs are not yet aware of — is that Salbutamol-only rescue therapy is no longer recommended even for mild intermittent asthma. The new first-line treatment for Step 1 is low-dose ICS-formoterol (e.g. budesonide-formoterol) used as needed. Every rescue puff also delivers an anti-inflammatory ICS dose — addressing the underlying inflammation at the same moment as the bronchospasm is relieved.
Step 2: SMART Therapy — The Standard for Most Persistent Asthma
SMART (Single Maintenance And Reliever Therapy) is the GINA 2026 preferred strategy for Steps 2–4. A single ICS-formoterol inhaler is used for both daily maintenance and as-needed rescue. On high-pollution days in Delhi, additional rescue puffs are not just bronchodilators — they are additional anti-inflammatory doses that directly counter pollution-driven airway inflammation. At Pulmovista Clinics, switching appropriate patients from traditional SABA rescue to SMART therapy is one of the most consistently impactful prescription changes I make.
| SMART-Compatible Inhalers Available in India | Components |
| Symbicort Turbuhaler | Budesonide + Formoterol — most widely prescribed; DPI format |
| Duoresp Spiromax | Budesonide + Formoterol — breath-actuated DPI |
| Fosterair / Vannair | Beclomethasone + Formoterol — extra-fine particle; excellent lung deposition |
| Bufomix Easyhaler | Budesonide + Formoterol — suitable for elderly and children ≥6 years |
Step 3–4: Add-On Therapies When SMART Is Insufficient
For patients who remain symptomatic on SMART therapy, add-on medications available at Pulmovista Clinics include:
• Leukotriene receptor antagonists (Montelukast): Particularly useful for patients with comorbid allergic rhinitis or aspirin-exacerbated respiratory disease — common in Delhi’s high-pollen, high-pollution environment.
• Tiotropium (LAMA add-on): For Step 4 patients — approved as add-on to ICS-LABA for adults with persistent symptoms, providing additional bronchodilation through a separate pathway.
• Azithromycin (low-dose long-term): For neutrophilic asthma — the pollution-driven phenotype — with anti-inflammatory and antimicrobial properties reducing exacerbation frequency.
Step 5: Biologic Therapy — When Standard Asthma Medications Are Not Enough
For patients who score 3–5 NO answers on this checklist — or who have had 2 or more severe exacerbations in the past year — biologic therapy assessment at Pulmovista Clinics is the appropriate next step. Biologics are precision-medicine injections that target the specific molecular pathways driving severe airway inflammation:
| Biologic Agent | Target / Best Patient Profile |
| Omalizumab (Xolair) | Anti-IgE — severe allergic asthma with elevated IgE; ideal for Delhi’s dust mite + pollen-sensitised patients |
| Mepolizumab (Nucala) | Anti-IL-5 — severe eosinophilic asthma; blood eosinophils ≥300 cells/µL |
| Benralizumab (Fasenra) | Anti-IL-5Rα — severe eosinophilic asthma; 8-weekly maintenance dosing |
| Dupilumab (Dupixent) | Anti-IL-4/IL-13 — Type 2 asthma + atopic dermatitis or nasal polyps |
| Tezepelumab (Tezspire) | Anti-TSLP — broadest eligibility; effective across all severe asthma phenotypes |
The Medication That Is Failing May Not Be the Prescription — It May Be the Technique
Before concluding that asthma medications need to be changed, one critical factor must always be assessed: inhaler technique. Studies consistently show that over 70% of asthma patients use their inhalers incorrectly — with errors that reduce drug delivery to the lungs by 50–80%. The most effective asthma medications in Delhi are useless if they are deposited on the back of the throat rather than delivered to the inflamed bronchioles where they are needed.
| ⚠ Most Common Inhaler Errors I Correct at Pulmovista Clinics ⚠ Dry Powder Inhaler (DPI) — inhaling too slowly: DPIs require a fast, deep inhalation to disperse the powder. Slow inhalation leaves the dose undispersed. ⚠ MDI without spacer: Without a spacer, up to 80% of the dose from a pressurised MDI hits the back of the throat instead of reaching the lungs. ⚠ Breathing out into a DPI before inhaling: Moisture from the exhaled breath clumps and ruins the powder dose loaded in the device. ⚠ Not holding breath after inhalation: Skipping the 10-second breath-hold significantly reduces lung deposition. ⚠ Not rinsing mouth after ICS use: Leads to oral thrush (candidiasis) and hoarseness — causes patients to reduce or stop their ICS, worsening asthma control. ⚠ Skipping the controller, using only the rescue: The single most common and most consequential error — treating symptoms without treating the underlying inflammation. At Pulmovista Clinics, every patient demonstrates their inhaler technique at every appointment. A 60-second technique correction can have more impact on asthma control than a complete medication change. |
Why Seeing a Respiratory Disease Specialist in Delhi Changes Everything About Asthma Medications
A respiratory disease specialist in Delhi brings something to asthma medication management that general practice cannot provide: the combination of specialist diagnostic tools, biomarker-guided prescribing, GINA 2026-current protocols, and deep familiarity with Delhi’s specific asthma triggers. At Pulmovista Clinics, here is what a specialist assessment changes:
1. Objective confirmation of diagnosis: Spirometry with bronchodilator reversibility confirms whether the diagnosis is asthma, COPD, dysfunctional breathing, or another condition — before a medication is prescribed or continued.
2. FeNO-guided ICS dosing: Fractional exhaled nitric oxide measurement tells me the exact level of eosinophilic airway inflammation — enabling me to set the ICS dose that matches the inflammation burden, rather than prescribing standard doses regardless of the individual patient’s biology.
3. Phenotype identification: Allergic vs. non-allergic, eosinophilic vs. neutrophilic, exercise-induced, aspirin-exacerbated — each phenotype requires a different medication strategy. Phenotyping requires allergy testing, blood eosinophil counts, FeNO, and clinical assessment that only a specialist can integrate meaningfully.
4. SMART therapy prescription: GINA 2026-aligned SMART therapy is still not universally prescribed in Delhi general practice. As a respiratory disease specialist in Delhi, SMART therapy is my standard prescribing for appropriate patients — not an advanced option.
5. Biologic therapy access: The five approved biologic therapies for severe asthma require specialist prescription following biomarker assessment. At Pulmovista Clinics, I conduct the full eligibility workup and prescribe all five biologics — providing access to treatments that are transformative for patients with severe, uncontrolled asthma.
6. Allergen immunotherapy: For patients with confirmed allergic sensitisation — modifying the underlying allergic disease through subcutaneous or sublingual immunotherapy reduces asthma severity over 3–5 years. This disease-modifying treatment is only available through specialist centres like Pulmovista Clinics.
When Asthma Medications Alone Are Not Enough: Pulmonary Rehabilitation at Pulmovista
For patients with severe or difficult-to-treat asthma — particularly those with significant breathlessness, exercise limitation, deconditioning, or anxiety — asthma medications are a necessary but sometimes insufficient solution on their own. At Pulmovista Clinics, Dr. Dixit Kumar Thakur integrates pulmonary rehabilitation as a complementary intervention for eligible asthma patients, recognising that the best pulmonary rehabilitation in India addresses the whole patient — not just the airways.
The best pulmonary rehabilitation Delhi has to offer — available at Pulmovista Clinics — includes breathing retraining (pursed-lip breathing, diaphragmatic breathing, ACBT), progressive supervised exercise training that desensitises patients to breathlessness, education on asthma medications and trigger avoidance, nutritional support, and psychological care for the anxiety and depression that frequently accompany poorly controlled severe asthma. For patients who have answered NO to 3 or more questions in this checklist and whose daily life is significantly limited by asthma, pulmonary rehabilitation alongside optimised asthma medications produces outcomes that medications alone cannot achieve.
| ✔ Pulmovista Clinics: Integrated Asthma Care — Medications + Rehabilitation ✔ Complete asthma medication review — GINA 2026 aligned, phenotype-guided, biomarker-informed ✔ SMART therapy initiation for appropriate patients — same appointment ✔ Biologic therapy assessment for severe uncontrolled asthma — Omalizumab, Mepolizumab, Benralizumab, Dupilumab, Tezepelumab ✔ Allergen immunotherapy for confirmed allergic sensitisation ✔ Inhaler technique assessment and hands-on correction — every appointment ✔ Best pulmonary rehabilitation Delhi — breathing exercises, exercise training, education, psychological support ✔ FeNO testing, spirometry, allergy panel — all on-site at Pulmovista Clinics ✔ Written personalised asthma action plan — including AQI 300+ protocol for Delhi patients Contact Pulmovista Clinics: www.pulmovista.com |
Conclusion: Your Asthma Medications Should Be Working — Let Pulmovista Clinics Make Sure They Are
Five questions. Two minutes. And the answers reveal whether the asthma medications your family has been relying on are doing their job — or whether you have been managing symptoms while the disease progresses unchecked underneath.
In 2026, there is no reason for uncontrolled asthma to be accepted as normal. The asthma medications available today — SMART therapy, biologic injections, allergen immunotherapy — are genuinely transformative. But they only transform outcomes when they are correctly prescribed, by a specialist who has done the diagnostic work to understand your specific asthma phenotype, your specific allergen triggers, and your specific challenge of living and breathing in Delhi.
At Pulmovista Clinics, that is exactly what Dr. Dixit Kumar Thakur provides. A specialist assessment that goes beyond the prescription pad. Medications chosen for your biology, not just your symptom description. And a long-term partnership — through Delhi’s worst pollution days, its dust storm seasons, its Diwali nights — to ensure that your asthma stays controlled not just today, but for years to come.
Use this checklist. Share it with your family. And if your score shows what I suspect it will — book your appointment at Pulmovista Clinics. Your lungs deserve better than ‘not hospitalised.’
FAQs-Asthma Medications and the Self-Check Guide
- I scored 4 NO answers. Does this mean my GP has been treating me incorrectly?It means your asthma is not well-controlled on your current treatment — which may reflect that the treatment needs stepping up, rather than that it was necessarily prescribed incorrectly in the first place. Asthma is a dynamic disease that often progresses over time, and the treatment that was adequate three years ago may no longer be sufficient today. Additionally, GINA guidelines have changed significantly — GINA 2026 recommendations differ meaningfully from guidelines of even 3–4 years ago, and many GPs have not yet updated their prescribing to reflect this. The right response to 4 NO answers is a specialist review at Pulmovista Clinics — not self-blame or GP-blame.
- I use my blue inhaler every day but my asthma feels 'under control.' Should I still see a specialist?Yes — immediately. Daily rescue inhaler use is one of the clearest markers of uncontrolled asthma according to GINA 2026. The feeling of control is a symptom-management illusion: the Salbutamol is temporarily relieving bronchospasm while the underlying airway inflammation continues unchecked, driving airway remodelling with every episode. Patients who use Salbutamol daily are at significantly elevated risk of severe, potentially fatal exacerbations — particularly during Delhi's pollution peaks. This is an urgent medication review situation at Pulmovista Clinics, not a routine check-up.
- My doctor says my asthma medications are working because I haven't been hospitalised. Is this the right measure?No — and this is a standard of asthma control that is far below what GINA 2026 considers acceptable. Avoiding hospitalisation is the minimum possible threshold — not evidence of good control. Well-controlled asthma means essentially no daytime symptoms, no nighttime waking, no rescue inhaler use beyond twice weekly, and no limitation of daily activities. If your current standard is 'not hospitalised,' the medication is providing crisis avoidance — not asthma control. A formal assessment using the 5-question checklist above, combined with spirometry and FeNO measurement at Pulmovista Clinics, will reveal the true picture.
- Is SMART therapy safe for long-term use in Delhi's pollution environment?Yes — SMART therapy has an excellent long-term safety profile supported by over a decade of clinical trial data. The ICS component (inhaled corticosteroid) is the same as used in traditional controller therapy — delivered more intelligently, with every rescue puff also providing anti-inflammatory coverage. In Delhi's high-pollution environment, SMART therapy is particularly well-suited because the as-needed rescue puffs on high-AQI days provide additional anti-inflammatory cover precisely when the inflammation burden is highest. Dr. Dixit Kumar Thakur monitors all Pulmovista patients on SMART therapy with regular spirometry and FeNO review to ensure optimal dosing over time.
- How do I book an asthma medication review at Pulmovista Clinics?You can book a consultation with Dr. Dixit Kumar Thakur at Pulmovista Clinics by visiting www.pulmovista.com or calling the clinic directly. Both in-person and teleconsultation appointments are available across Delhi NCR. When booking, mention that you are coming for an asthma medication review — this ensures the appropriate appointment duration is allocated and that spirometry and FeNO testing are arranged for the same visit. If you have answered NO to 3 or more questions in this checklist, please request an urgent appointment.